 China
China  Africa
Africa 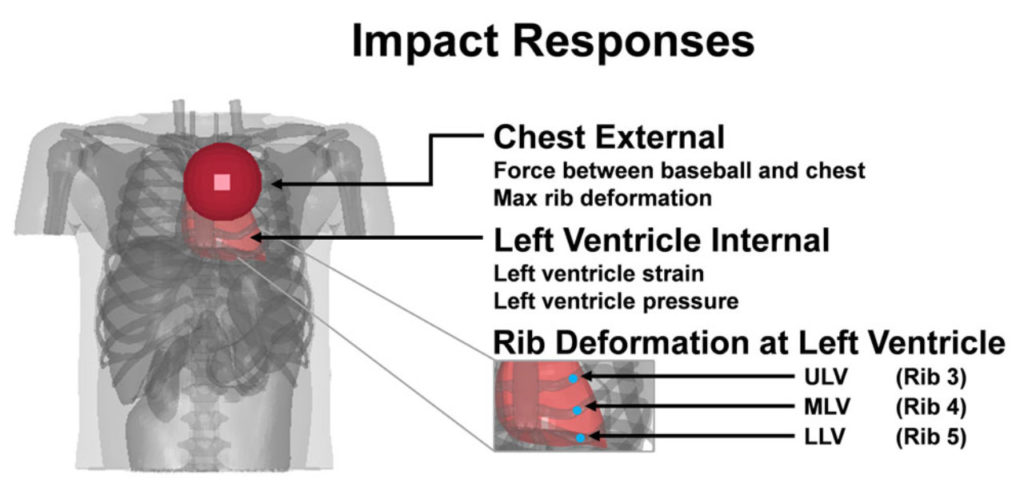
Case 93: Tachycardia Leading to Ventricular Fibrillation
Layne Kerry, Janice Rymer
A 47-year-old man attended the emergency department complaining of shortness of breath and palpitations. He had felt generally unwell over the preceding weeks, with a dry cough, dyspnoea, unintentional weight loss and fatigue. His past history included a resected gastric carcinoma (T4, N1, M0), and asthma, which had been present since childhood. He took 40 mg omeprazole OD and used a salbutamol inhaler several times daily. He had previously worked as a laboratory technician but was currently unemployed. He had no recent travel history. He was a current smoker with a 40 pack year history and did not drink alcohol.
Catheter Ablation of Ventricular Fibrillation and Polymorphic Ventricular Tachycardia
Amin Al-Ahmad, Carola Gianni, Andrea Natale
Ventricular fibrillation and sustained polymorphic ventricular tachycardia are malignant arrhythmias resulting in sudden cardiac death. Sudden cardiac death is a leading cause of death in the industrialized world, with Ventricular fibrillation and polymorphic ventricular tachycardia accounting for up to one-third of all cases. Though the majority of Ventricular fibrillation/polymorphic ventricular tachycardia occurs in structurally abnormal hearts, there is a subset of individuals resuscitated from sudden cardiac death with no structural heart disease. In some of these patients, Ventricular fibrillation/polymorphic ventricular tachycardia is triggered by premature ventricular complex that can be mapped and targeted by catheter ablation to prevent subsequent episodes. Patients with idiopathic Ventricular fibrillation are patients with prior history of resuscitated sudden cardiac death, but without structural heart disease or electrocardiographic abnormalities.
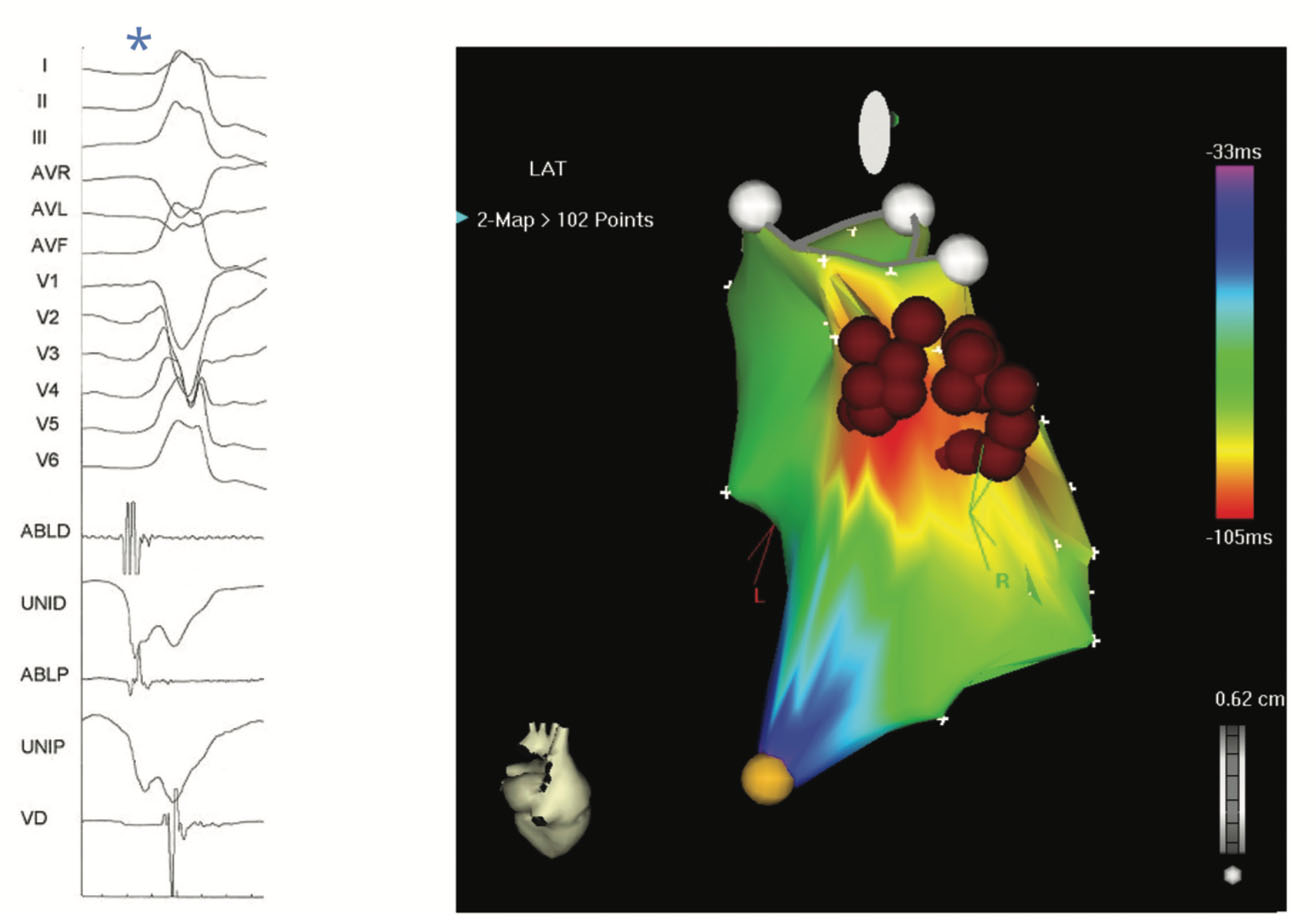
Figure 24.4 PMVT-triggering PVC originating from the RVOT myocardium.
Sudden cardiac death: Prevalence, pathogenesis, and prevention
Published in Annals of Medicine
Dr Martina Montagnana, Giuseppe Lippi, Massimo Franchini, Giovanni Targher, Gian Cesare Guidi
Commotio cordis, or non-penetrating chest wall impact, is a mechanical induction of heart rhythm disturbances in the absence of corresponding structural damage. Reported with increasing frequency in young individuals participating in some sport activities, it may cause SCD by acute initiation of ventricular fibrillation 89. Commotio cordis is the second leading cause of death in young athletes and most events are caused by blows from projectiles, baseballs, or lacrosse balls, with a substantial proportion, nearly 40%, occurring despite the use of a chest protector 90.
Particularly, baseball impacts induce ventricular fibrillation when directed at the center of the left ventricle during the vulnerable portion of repolarization just prior to the T wave peak 90. The electrophysiological changes have been attributed to mechanoelectric feedback, and particularly to the recruitment of stretch-activated ion channels. However, the underlying mechanisms by which a mechanical impact results in ventricular fibrillation remain mostly unknown 91. Li et al. 91 demonstrated that the region of impact is characterized by different types of cellular responses, including generation of a new action potential, and shortening or lengthening of action potential duration.
Developing commotio cordis injury metrics for baseball safety: unravelling the connection between chest force and rib deformation to left ventricle strain and pressure
Published in Computer Methods in Biomechanics and Biomedical Engineering
Commotio cordis is a sudden death mechanism that occurs when the heart is impacted during the repolarization phase of the cardiac cycle. This study aimed to investigate commotio cordis injury metrics by correlating chest force and rib deformation to left ventricle strain and pressure. We simulated 128 chest impacts using a simulation matrix which included two initial velocities, 16 impact locations spread across the transverse and sagittal plane, and four baseball stiffness levels. Results showed that an initial velocity of 17.88 m/s and an impact location over the left ventricle was the most damaging setting across all possible settings, causing the most considerable left ventricle strain and pressure increases.
Sudden cardiac death in sports: could we save Pheidippides?
Published in Acta Cardiologica
Hereditary diseases under the age of 35 are the most common underlying heart disease, leading to sudden cardiac death (SCD) in competitive sports, while in older people, atherosclerotic coronary artery disease (CAD) is the main cause. The following preventive measures are recommended: (a) The pre-participation cardiovascular screening, (b) the genetic testing, (c) the use of implantable cardioverter-defibrillator (ICD), (d) the prohibition of doping in sports, (e) the prevention of ‘exercise-induced’ cardiac complications, (f) the reduction of high-risk factors for CAD, and (g) the use of cardiopulmonary resuscitation.